Viscount Younger was new to the post and when questioned on the subject of suicides by MP Debbie Abrahams, he…
Read More


Viscount Younger was new to the post and when questioned on the subject of suicides by MP Debbie Abrahams, he…
Read MoreWhen Viscount Younger was Parliamentary Under Secretary of State he said in select committee on 18th January 2023: “Could I…
Read More
Up to 300 parents a year may be dying by suicide under the CMS system STOPSuicides UK analysis of official…
Read More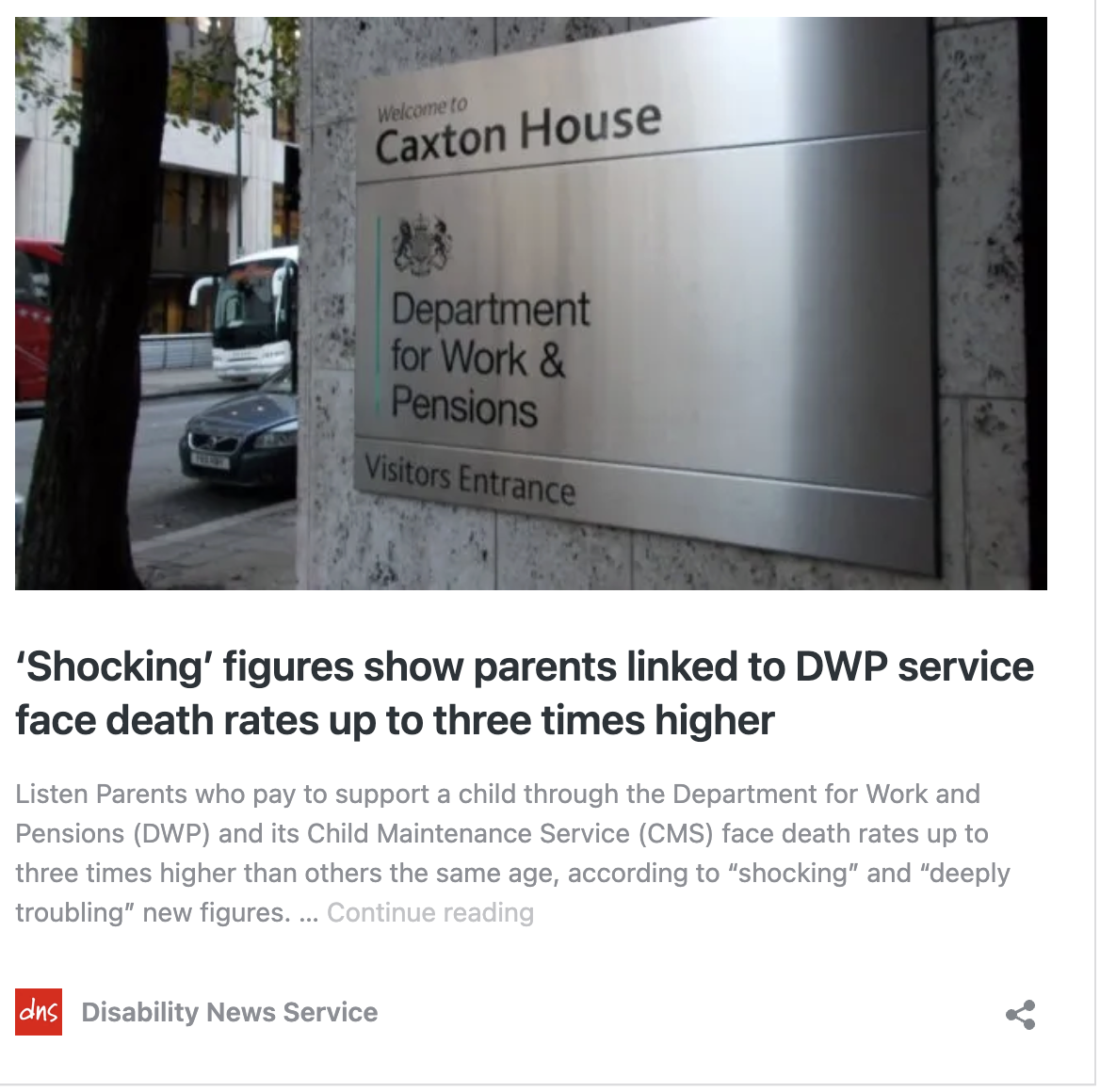
A shocking report published by the Disability News Service points to the impact on Paying Parents (PPs) and their children…
Read More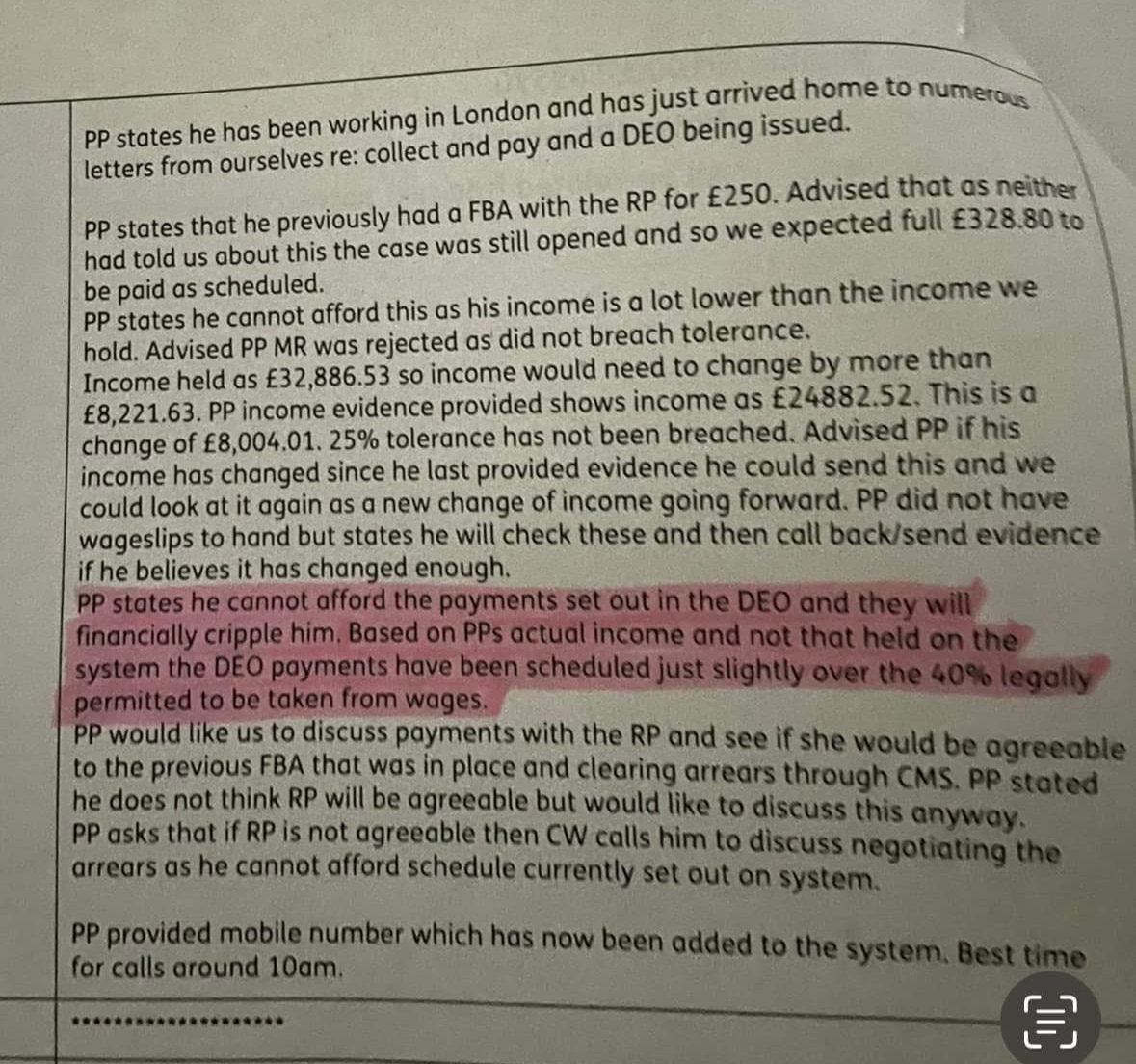
The DWP denies there is a link between its actions and people who take their own lives. Check out this…
Read MoreViscount Younger stated: “Thank you for your further email of 6 September to the Minister for Lords. Government Ministers receive…
Read More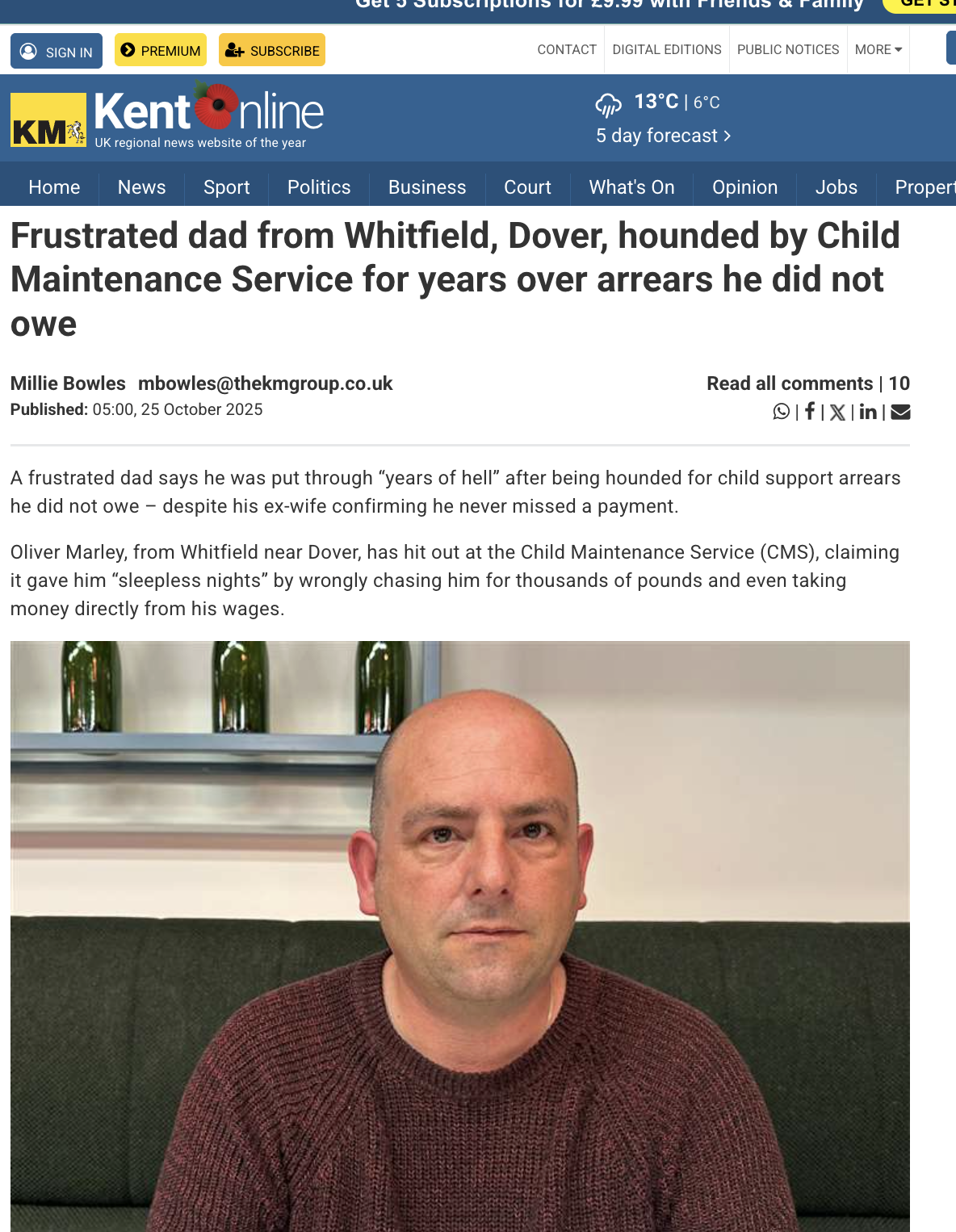
An all too commonplace tale of maladministration at this infamous . The impact on mental health when a victim has…
Read More
IT JUST TAKES SECONDS for people stressed out by Child Maintenance Service to request the data that the CMS holds…
Read More
“STOPSuicides UK is investigating failures in the CMS IT systems that have stressed both RPs and NRPs. In analysing the…
Read More
STOPSuicides UK 6th September 2025 Baroness Sherlock OBEMinister of StateDepartment for Work and PensionsCaxton HouseTothill StreetLondon SW1H 9DA Subject: Contradiction…
Read More
This is the CMS Narrative: 77. The Government recognises that some paying parents face difficult circumstances and may be in…
Read More